
The Brainstem
The brainstem is ancient. All our ancestors ate and drank (chewed and swallowed). The brainstem links to the heart and lungs (blood and air) and also monitors glucose levels.
The brainstem receives data from the digestive system (and elsewhere):
* tongue
* stomach
* duodenum
* liver
It then transmits this information further into the brain i.e. to the hypothalamus.
Fluid Regulation
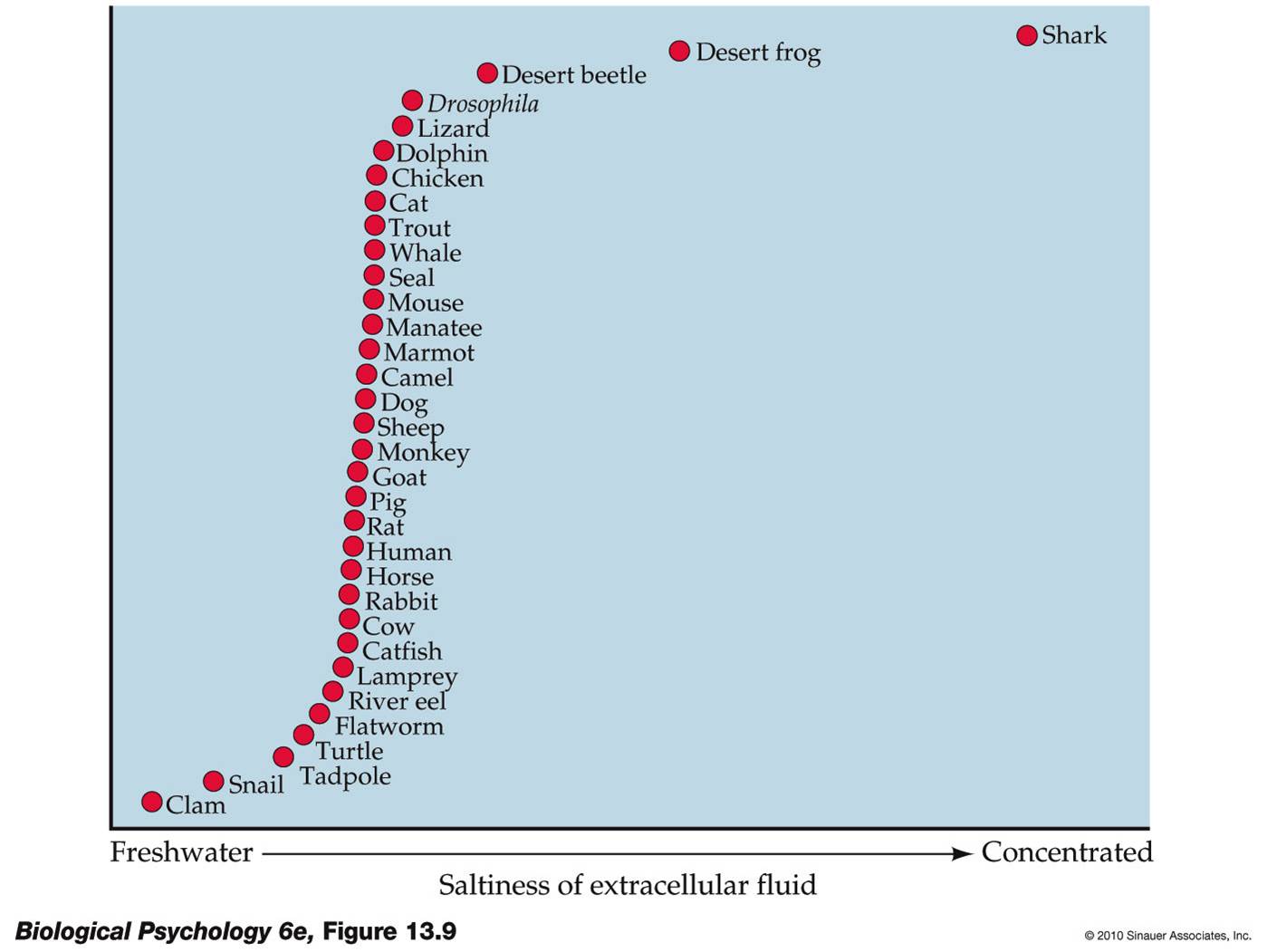
Extracellular fluid is like seawater.
Daily Water Balance
* Intake of water - from water itself and from food (about 2.5 litres)
* Output of water - through urine, evaporative loss and faeces (about 2.5 litres)
There is a balance here.
Fluid Balance
Intracellular fluid accounts for about 67%. Extracellular fluid accounts for the rest. There are different types of extracellular fluid:
* Interstitial fluid (26%)
* Blood plasma (7%)
* Cerebrospinal fluid in the brain (approximately 1%)
If the levels of these drop, you get thirsty. Intracellular fluid and blood plasma are the most important.
Osmosis ensures that there is an equal salt concentration on both sides of the membrane. This is shown in the diagram below.

With plenty of water, cells work well. If they have too much, they rupture as chemical reactions fail. Little water = lots of salt.
Outside of a cell there is lots of water and few solutes. Osmosis brings the water into the cell and ensures there is the same concentration on both the inside and the outside.
Blood Plasma
Blood plasma is critical to the heart. Without enough blood, the heart is unable to pump effectively. There is some flexibility however this is limited. Too much plasma (and therefore pressure) causes blood vessels to burst.
A hangover is losing cerebrospinal fluid in the brain, therefore you need lots of water!
Two types of thirst
There are two types of thirst. These are called volumetric thirst and osmometric thirst. Volumetric thirst is caused by loss of blood plasma, whilst osmometric thirst is caused by the loss of intracellular water. Feeling thirsty leads you to seek out water - this a behavioural.

In volumetric thirst you lose water through serious blood loss and diarrhoea. Osmometric thirst is caused by lack of water e.g. through a salty meal.
Osmometric Thirst
Osmometric thirst is caused by not having enough water in your cells. The cells begin to shrink. Specialist neurons are able to spot this. These are called osmoreceptors. Cell shrinkage leads to a change in the rate of neuron firing, this is shown in the diagram below.

The diagram below shows circumventricular organs. Note the lamina terminalis.

The anterior cingulate cortex is the most primitive cortex in the limbic system. It is responsible for the sense of thirst. This area of the brain gives you the feeling of a dry throat even though you're throat isn't actually dry. This is also known has motivational unpleasantness.


When you are running short of water, the anterior cingulate is aware. It gets more active which makes you thirsty. Once you have had a drink, the lamina terminalis settles down after about 20 minutes.
Volumetric Thirst
Volumetric thirst is caused by a lack of blood plasma. This occurs through loss of blood (and blood pressure), diarrhoea and vomiting. It means you have a lack of salt within your bodily fluid.
Atrial Baroreceptors detect the stretchiness (or lack of) of arteries. They release atrial natriuretic peptide (ANP). When blood pressure drops, less is produced. This inhibits drinking and boosts the kidneys. The less ANP there is, the thirstier you get.

Vasopressin is a peptide hormone released by the posterior pituitary gland. It is an anti-diuretic hormone (ADH) which instructs the kidneys to reduce the flow of water to the bladder.



The diagram above shows hormones, their relationship with enzymes and the effects caused. Remember that the circumventricular organs is the lamina terminalis! The lamina terminalis spots thirst.
Both types of thirst (volumetric and osmometric) activate thirst in the same place/area. This is shown in the diagram below.


Food Regulation
The average American eats 3,800 calories a day. Half of the US is clinically obese whilse 3% of US adolescents suffer from anorexia or bulimia nervosa.
Although food provides energy, about 33% of energy is food is lost during digestion. 55% is consumed by metabolism e.g. maintaining membrane potentials and heat production etc. The last 12% is used for active behaviour.
Long-term satiety
Fluctuating body weight adjusts over a long-term basis. Force-fed rats will reduce their food intake once they are permitted to do so. This shows that it can't be weight that is measured - how does your body know? Your body knows when your hormones and fat cells are full.
Energy Storage
Glucose is the principle sugar, therefore it must be stored inertly. Glucose is converted into glycogen. This is called glycogenesis. You don't keep glucose in your system as it is unhealthy. Glycogen is stored in the liver and muscles. Every time you convert glucose into glycogen, you lose some - it is not a perfectly efficient process. Glycogenesis involves insulin which is a peptide.
Insulin and Satiety
Newly released insulin allows for the instant use of glucose (and storage of the rest). Glucodetectors in the liver, signal the 'nucleus of solitary tract' (NST) which is in the hypothalamus. Too much glucose causes you to secrete insulin.

See the diagram above. Leptin is released by fat cells, ghrelin by the stomach and PYY by the gut. A combination of all of these, drives apetite. The signals produced go to the brainstem or hypothalamus.
The dual-centre hypothesis states that there is one area for hunger and one for satiety. This hypothesis is far too simplistic.

In the lateral hypothalamus, lesions cause Aphagia (refusal to eat). Whereas lesions/damage in the ventromedial hypothalamus cause obesity. The latter has been found in research involving rats, dogs and humans.
The diagram below, shows what occurs when there are lesions in the ventromedial hypothalamus.

The satiety centre is where the arrow points. The satiety centre is the part that tells you that you are full. Therefore the arrow points to the fact that the lesion has destroyed this.
It is not just insulin that effects satiety. All four hormones listed previously are important (leptin, ghrelin and PYY). Ghrelin releases growth hormones.
Leptin
Leptin is a chemical secreted by well-nourished fat cells i.e. it tells you not to eat anymore. Certain mice are unable to produce leptin this makes them obese.

Both mice in the picture above are obese due to being unable to produce leptin. The mouse on the right however is injected with leptin on a daily basis. The mouse on the left weighs 67g whilst the one on the right only weighs 35g.
However, when injecting leptin into rats it increases their aggression.
Ghrelin
Ghrelin releases growth hormones. When the stomach is empty then it secretes ghrelin but when it is full it secretes hydrochloric acid. Ghrelin increases before meals and the levels drop immediately after a meal is eaten. It is only when the stomach is empty that you need to eat.
If you inject ghrelin into the cerebral ventricles you get a massive increase in apetite.
PYY3-36
PYY is secreted by both the small and large intestines. You have low blood levels prior to meals. Injecting PYY curbs apetite in both humans and rats. Therefore it has the opposite effect to ghrelin.
When the hypothalamus picks up on PYY it knows that you have food in your gut/intestine. The diagram below shows peptic hormones.


Leptin and insulin are longer term chemicals. They deal with the consequences of your reserve e.g. leptin - how much fat you have. They activate appetite-suppression areas and inhibit appetite-increasing areas.
Ghrelin and PYY are short-term chemicals which are based entirely on whether you have eaten (immediate).
Over/under eating
Starvation is worse than overeating (it is fatal in short-term) and is evolutionarily more likely. We have evolved to obtain/store food - we eat when empty, not when hungry. Everyone eats more than they need to. We enjoy high calorie foods therefore are predisposed to putting weight on.
What stops eating?
1) Short-term satiety - feedback from food you have yet to swallow, eyes, nose, mouth and the contents of
your gut.
2) Long-term satiety - fatty tissue (eating more has an effect - build fatty tissue).

The image above shows a study by Weingarten & Kulikovsky (1989). Rats were given one of two diets:
1) usual diet - gradually eat more
2) completely new diet - ate more from the start

The hypothalamus monitors peptide hormones in the blood.
Weight Loss
Most programs are unsuccessful. Weight loss is rapid, then it declines, then halts. When the diet ends you then rapidly gain weight and you are back to the starting point.
Who gains weight?
Some prefer high calorie foods, some cultures are more prone. Output such as exercise is important.
Eating Disorders
50% of the US are obese. Anorexia Nervosa accounts for 1.5% - here there is evidence of abnormal peptide levels. Anorexics find it hard to increase their desire to eat more. Bulimia Nervosa also accounts for 1.5% and relates to a lack of nutrient reserves.
So, fluid and food intake is now done. Just over 9 hours till the exam so best get cracking on the next topic (reproductive behaviour).
xoxo












































